

By Ralph R. Gregory, D.C.
Vol. 3, No. 1, June, 1981
THE PROBLEM
Mechanically inept adjusting is too frequently used to restore the C-1 subluxation’s misalignment factors to the vertical axis. Adjusting a C-1 subluxation as the case with any motor skill is based on the use of relevant anatomic and mechanical principles of human motion, i.e., kinesiology. The adjuster who seeks to improve his skills can achieve a higher level of performance by understanding and applying basic kinesiological principles to the adjustment. The purpose of this paper is to discuss some of these kinesiological principles as they relate to the C-1 adjustment.
Greater skill is required to adjust the C-1 than any other vertebra in the spinal column. Anatomically, the load bearing responsibility of the occipitalatlanto-axial facets is different from the other segments due to the absence of a disk between C-1 and C-2. The facets are crucial to structural stability in the area.1 Neurologically, the occipital-atlanto-axial complex is different also, because of the close proximity to the brain stem and the medullary structures; more space is allocated for the spinal cord to reduce impingement by any bony structures. The requirement for structural stability and for a reasonable amount of movement for the skull and the cervical unit make this segment of the spinal column the most unique and demanding for the adjuster.
Steindler reports that the movement of the intervertebral joints is contingent upon the shape of the articular facets.2 The facets, therefore, determine the type, the direction and the range of motion of the subluxation. According to White and Panjabi, in the cervical spine the facets are located 45° to the frontal plane with 0° rotation to the frontal plane. In the thoracic spine the facets are positioned at 60° to the frontal plane with 20° of rotation to the frontal plane, and with the lumbar spine the facets are positioned 90° to the frontal plane and rotated 45° to the frontal plane.3 The expectation is that with each of the three major spinal units the intervertebral movement will vary with the angle set of the facet. As the load bearing responsibility shifts from facet to disc at the various levels of the spine the combinations of movement become more restrictive between the vertebrae. The number of reduction pathways is also reduced which would tend to lessen the adjusting skill required to reduce the subluxation. By the same logic, as the facets assume more of the load responsibility as is found in occipital-atlanto-axial complex where there is no disc, adjusting requires skill and proficiency due to the infinite number of reduction pathway combinations.
There is also evidence to support the theory that a C-1 subluxation stresses the entire spinal column. In a 1978 study by Seemann it was found that without exception that a patient who had a C-1 subluxation as determined by x-ray, also exhibited pelvic distortion, a short leg, and spinal imbalance.4 The spinal stress is the result of a neurological imbalance between the facilitatory and inhibitory mechanisms of the reticular formation of the brain stem. Spastic contracture of the extensor muscles is caused from the loss of inhibitory control as C-1 moves outside its normal range of motion. This abnormal movement is thought to be responsible for the C-1 syndrome: pelvic distortion, short (contractured) leg and spinal imbalance. The Seemann study also reported that alleviation of the C-1 syndrome necessitates correcting the C-1 misalignments. At no other level of the spinal column can correcting a subluxation remedy the syndrome.
MEASURING METHODS
An analysis of the C-1 adjustic motor skill can be divided into two major categories: anatomic and mechanical. It is with the mechanical that this paper is chiefly concerned. An analysis of both categories is lengthy, and would defeat the purpose of this paper which is to briefly acquaint the C-1 adjuster with a few basic mechanical principles that should aid in more efficient and easier adjusting.
The most conclusive proof of the degree of efficient performance is the post x-ray. Thousands of x-rays (taken immediately after the C-1 adjustment) have been analyzed to determine the degree of performance. This study has been carried out for over thirty years. Adjustic innovations have been examined to determine their value in the motor skill, adopted, modified, or rejected. The mechanical contents discussed in this paper have all been subjected to post x-ray analysis.
Another valuable tool for determining efficient performance of the C-1 motor skill is the anatometer which measures the amount of spinal column and bodily distortion caused by a C-1 subluxation. Because the anatometer measures the correction, or degree of correction following an adjustment of C-1, the instrument can indicate dramatically if a correction of C-1 has occurred.
Videotapes provide another tool when used in practice sessions. Because these tapes can be stopped or “frozen” at any point, a detailed study can be made of each step for any adjustic phase.
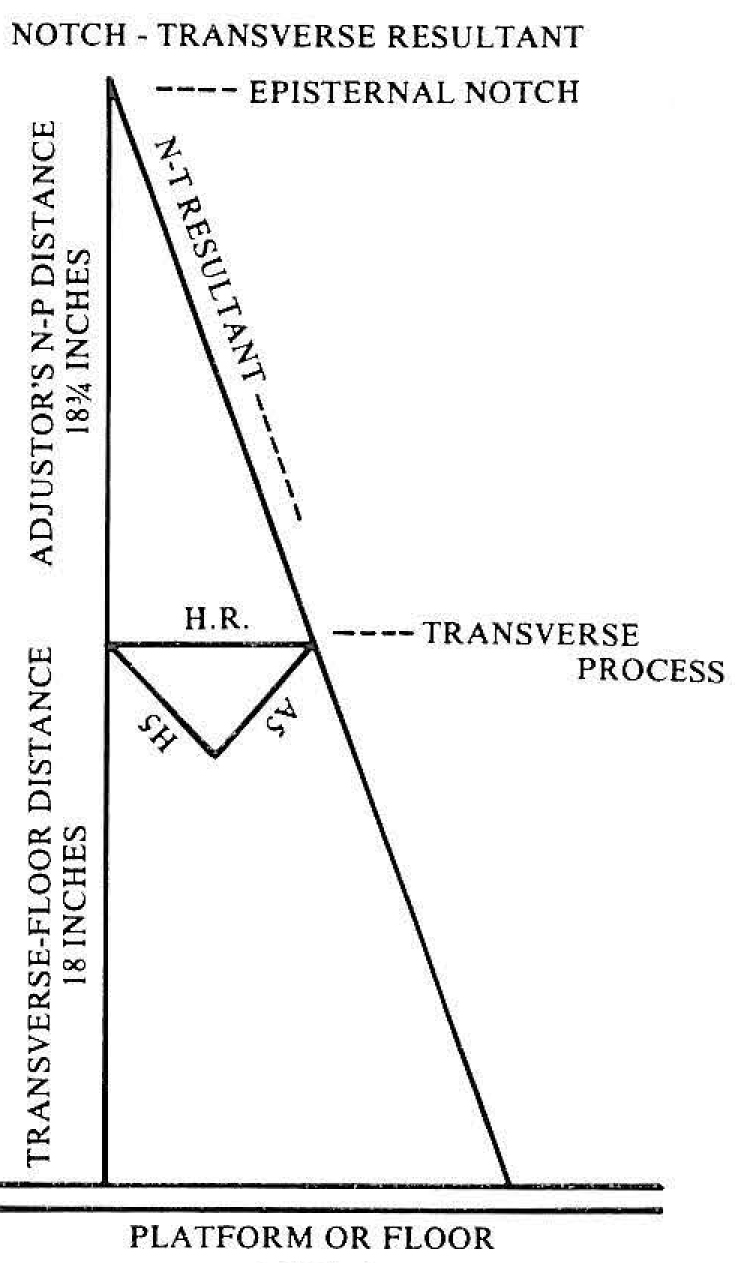
Figure 1: The reduction pathway (N-T Resultant) computed from x-rays and the adjuster’s episternal notch to transverse distance for a C-1 subluxation requiring vertical and horizontal vectors of 5 inches.
Another device of great value in practicing the adjustic motor skill is the light pattern study. Because all adjustments must be delivered so that the action lines, or parallel forces, of the adjuster’s body are coplanar with the notch-transverse resultant (reduction pathway) to achieve rectilinear motion (Fig. 1), the light pattern device is especially valuable in conditioning the adjuster’s body planes to the reduction pathway of the C-1 subluxation. A harness is attached to the adjuster’s body which contains two small spotlights that represent his parallel forces. In a dimly lighted room, the adjuster may study his movements throughout the several phases of the adjustment, determining their accuracy and the alignment of his parallel forces to the reduction pathway in the final or kinetic phase.
DISCUSSION
Gowitzke and Milner define a motor skill as a group of simple, natural movements combined in a new or unusual manner to achieve a predetermined objective.5 The C-1 adjustic motor skill is a series of simple and natural angular motions performed to achieve rectilinear or straight line motion in the final or kinetic phase of the adjustment along a predetermined pathway computed from the x-ray film analysis. This predetermined pathway is the reduction pathway along which motion must be expressed if correction of the C-1 subluxation complex is to be achieved. Each C-1 subluxation has its own reduction pathway which is represented by the notch-transverse resultant (Fig. 1).
The simple, natural angular movements of the adjuster are referred to as the potential phases of the adjustment. They are movements, the total of which are designed to produce linear motion in the final or kinetic phase in which the adjustment is delivered.
MOTION
Motion has been described as the change of position of an object, or, more technically, as the act or process of changing position or place with respect to some reference point. Rasch and Burke define three general types of motion: Rectilinear or translatory, angular or rotatory, and curvilinear. Rectilinear motion takes place when every particle of a body moves the same distance a long a straight line which is parallel to the path of every other particle. In angular or rotary motion, each particle of a rigid body moves in a circle or along the arc of a circle. The center of rotation or “axle” of the rotation may either be within the volume of the body, as in the case of a pirouetting dancer, or outside the body, as in the case of a gymnast swinging on the flying rings.6
These definitions of motion should alert the adjuster to the importance of using care and control when he exercises the potential phases of the adjustment. Care and control are so essential to his expression of rectilinear motion in the kinetic phase. To express rectilinear motion, the adjuster must know the external reference points, and be conscious of the joint centers of motion about which he moves in performing the potential phases. He should also be aware of the degree to which he moves about any given joint or axis of motion.
LOCK-ACTIONS
The use of lockactions aid the adjuster in achieving the required body balance and muscular control needed to produce rectilinear motion. Anderson defines a body lock-action as “putting a (body) part into a position which will automatically stabilize other parts of the body and lead to a more efficient action with a minimum of effort”.
Anderson states that the first of these two reflex actions, the neck-lock action, is accomplished by pulling the chin inward which straightens the cervical spine, stimulates retraction of the shoulders, and stabilizes the spinal column. The second, or foot-lock action, according to Anderson, is initiated by turning the feet medialward with the plantar surfaces in contact with the supporting surface; some pressure (weight) therefore is on the soles of the feet and the act is executed from the heel. It is this pressure on the plantar surfaces of the feet that activates the reflex action, stimulating a chain of muscular action upward throughout the adjuster’s body. The ankle and knee joints automatically lock, maintaining stability.7
The importance of the neck-lock action to the adjuster, other than balancing and positioning his shoulder level and spinal lever, is that it allows for easier and more complete contraction of his triceps brachii because the adjuster’s spinal column, chest, and head are stabilized. The reflex serves, furthermore, to protect the adjuster against whiplash during the adjustic act.
Another lock-action, the hip lock, maintains the adjuster’s pelvic lever at right angles to his spinal lever. This act is executed in the first, or approach, phase of the adjustment. In performing the phases of the adjustment, the tendency for the adjuster’s pelvic lever to turn about the lumbo-sacral joint is great, particularly when he advances his leg to establish the A-P distance of his base of support. If his pelvic lever rotates about his lumbo-sacral joint, his body shortens on the side of the forwardly placed foot, curving his spinal lever. Consequently, curvilinear motion is expressed in the kinetic phase of the adjustment, and the parallel forces turn from the reduction pathway. This error prevents reduction of the C-1 subluxation, especially of rotations and high lines of drive.
These lock-actions are frequently overlooked by the adjuster. As a result a loss of synergic action takes place in the adjuster’s body which leads to difficult performance of the motor skill and curvilinear motion in the final phase because of unbalanced muscular motion.
The action lines, or parallel forces, of the adjustic motor skill may be compared to the sights on a rifle. An adjustment, like a rifle, is aimed at a target. In the case of the rifle, the alignment of the sights determines accuracy; in the case of an adjustment, the adjuster’s alignment of his parallel forces decides if the energy generated by the motor skill enters the target (transverse process) along the reduction pathway prescribed by the film analysis. Control of joint motion, muscular balance, and stability are essential elements for obtaining efficient performance.
FORCE:
Force is frequently defined as a push or pull exerted to overcome resistance. Force is the instigator of motion. Everything that moves does so because a force is applied. The direction of the force, its magnitude, and the point of its application are the three most important aspects of force.
Force is a vector quantity because it possesses both magnitude and direction. Having these characteristics, it can be dangerous if misused, uncontrolled, or misdirected. It is the element that can make adjustments dangerous. Uncontrolled force in the C-1 adjustment produces depth which, if it exceeds the resistance offered by the subluxation, prevents reduction of the C-1 vertebra about the occipital condyles, transferring the excess force to the superior articulating surfaces of C-2. A kinking of the cervical spine at its weakest point – the atlas-axis articulation – results. This is very traumatic to the patient, because it increases the disequilibrium of the cervical spine, ultimately causing more subluxation. The skill of the C-1 adjuster is predicated on his ability to control and direct force.
Adjustic force is initiated by contracting the triceps brachii muscles along their line of pull. The line of pull is a straight line between the insertion of the muscle in the olecranon process of the ulnar and the origin of the long head in the infraglenoid tuberosity of the scapula. The direction of the line of pull (in the adjustic posture) is upward and somewhat medialward.
Muscles can pull from origin to insertion or from insertion to origin, a concept known as functional reversibility.8 The customary function of the triceps brachii is to adduct and extend the forearm; in the adjustic act, this function is reversed so that the inertia of the shoulder joint can be overcome.
The triceps muscle has the pulley action of a biaxial (two-joint) muscle. That is, it acts over the shoulder and elbow joints. A characteristic of a biaxial muscle is that it is too short to permit complete movement at the same time of both the joints it crosses. In the C-1 adjustic motor skill, the action of the triceps is concentrated at the shoulder joints.
Kinesiologists explain that the pectoral or shoulder girdle can be compared to a three-link chain. Movements at the glenohumeral joint are always accompanied by accommodating movements of associated osseous structures.9 If accommodation did not occur, the primary movement would be inhibited. In the C-1 adjustment the primary movement is the upward and inward movement of the humeri, initiated by the triceps brachii contraction as the adjuster contracts the muscles from a point about two inches below the glenohumeral joints. To obtain maximal action in the primary movement, the shoulder girdle must compress, the scapulae move medialward, and the episternal notch slightly extend.
The principle of the transfer of momentum states that the body is frequently put into motion by transferring momentum from a part of the body to the total body mass.10 The efficient adjuster utilizes this principle when he contracts his triceps brachii, which action compresses his shoulder girdle and overcomes its inertia. Momentum is thereby transferred to his body mass. At the moment of shoulder girdle activation, potential energy is converted into kinetic energy.
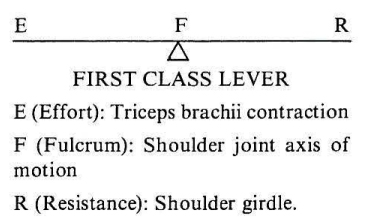
Figure 2: E (Effort): Triceps brachii contraction, F (Fulcrum): Shoulder joint axis of motion, R (Resistance): Shoulder girdle.
In terms of levers, the shoulder girdle is the resistance, or the load to be moved, the glenohumeral joints are the fulcra, and the contracting triceps brachii are the effort. As used in the adjustic action, this constitutes a lever of the first class: effort, fulcrum, and resistance (Fig. 2).
Efficient movement in a motor skill requires that levers having the largest mass possess the greatest inertia, and therefore should move first in the sequence of movement. Smaller levers, because they possess less inertia, should move later in the sequence.11 The lever with the greatest mass in the adjustment is the shoulder lever; therefore, it should move first in the adjustic action. The elbow, composed of smaller levers, should move after the shoulder lever in the sequence. When the elbows move first, too little efficient action results, because far less momentum is transferred to the adjuster’s body mass. Consequently, the adjuster’s body does not back up the adjustment, and little, if any, follow-through is expressed. Loss of vertebral reduction results. For these reasons, so-called recoil adjusting is a less effective means for correcting C-1 subluxations.
It should be clear by now that the resistance to be overcome by the adjustic motor skill is not the resistance offered by the C-1 misalignment factors; the resistance is the shoulder girdle which represents a relatively large load for the triceps to move. This load-resistance is greater than that offered by any C-1 subluxation.
It should be mentioned that speed of muscle contraction is of little value in overcoming resistance. In fact, speed violates the principle that the greater the speed of contraction, the less force generated or load moved and the greater the load, the less the velocity of shortening.12 Maximal contraction of the triceps is the requirement for efficient performance. To obtain maximal contraction, however, shoulder girdle resistance must be overcome. If the load (shoulder girdle) is equal to the force (triceps contraction), the result is zero.
If the adjuster consciously relaxes his shoulder musculature just prior to contracting his triceps, he will reduce the resistance to the triceps effort. At the exact moment of triceps contraction, the adjuster should allow his shoulders to move slightly posterior while at the same time squeezing them medialward. These resistance-reducing actions must be timed with the triceps contraction. Resistance is reduced because these actions start the movement of the associated osseous structures – the clavicles, scapulae, and the episternal notch extension – immediately prior to the triceps contraction.
The tendency for adjusters to tighten their shoulder musculature is quite common. When they do this, they increase resistance to the triceps effort. Until their triceps muscles are sufficiently developed, they can practice the resistance-reducing methods described above. Feedback can be obtained by practicing against a door-jamb or other immovable structure. If the adjuster rolls-in, places his contact-hand pisaform bone against the door-jamb and contracts (pulls) his triceps muscles from a point about two inches below his shoulder joints, his shoulder girdle will be compressed, forced backward and inward. This is the desired action in the C-1 adjustment. If it proves difficult, it is being done incorrectly.
The concept of overcoming shoulder girdle resistance appears difficult for adjusters to master, because they think in terms of the vertebrae, or the subluxation, as the resistance to the C-1 adjustment. Therefore, they direct the force into the subluxation. If they understand that the true resistance is their own shoulder girdle, they will direct the adjustic force into it, not into the patient’s neck. Furthermore, the adjustic force is controlled and more accurately directed, thus more effective. It can be adapted to the degree of subluxation resistance which varies with different cases. Trauma to the patient is avoided, because any force that too greatly exceeds the resistance of the subluxation is traumatic to the patient. It may be compared to using a crowbar to move a pebble.
An efficient C-1 adjustment, therefore, is not accomplished by entering a direct force into the patient’s neck, whether that force is delivered manually or by an adjusting modality. A directly applied force to the C-1 vertebrae can easily exceed its resistance which is small if all the conditions are compiled with. A directly applied force can move C-2 laterally as a unit when the desired action is to move C-1 about the condyles of occiput by moving it about the superior articulating surfaces of C-2, either down and around or up and around. Direct force tends to kink the cervical spine, if excessive, at the atlanto-axial articulation which blocks subluxation reduction, and may increase it.
A common misconception shared by many adjusters should be mentioned. This erroneous concept is that the forearms of the adjuster are forced outward by the triceps contraction against the locked or roll-in position of the hands. Two reasons argue against this concept: (1) that it uses the adjuster’s elbows as the primary lever to overcome, and (2) that it obviates the concentration of bilateral forces at the pisaform bone of contract hand.
BASE OF SUPPORT:
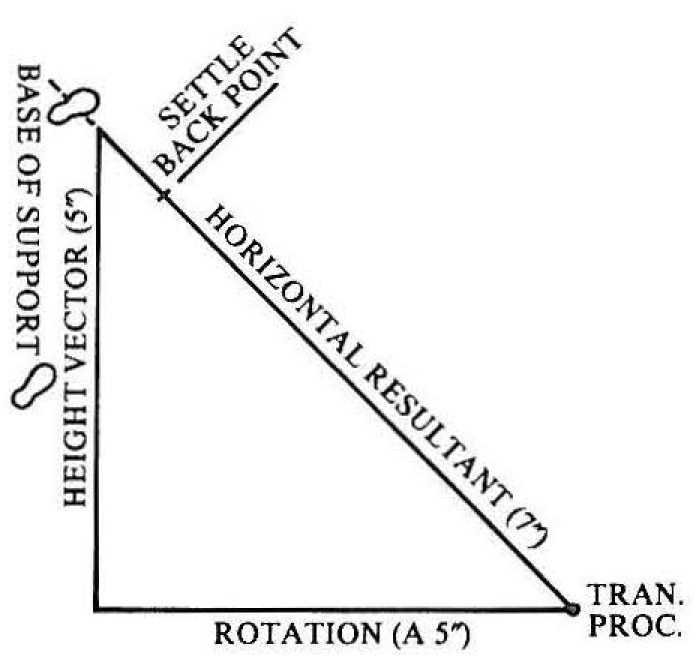
Figure 3: Aligning the adjuster’s feet (base of support) to the horizontal resultant.
Accurate alignment of the adjuster’s base of support to the horizontal resultant (see Fig. 3) of the C-1 subluxation is vitally important to the control of his center of gravity. Groves and Camaione define a base of support as the points in contact with the supporting surfaces and the two dimensional area between those points at contact.13 In the adjustic motor skill, the dimensions of the base of support are determined from the length of the horizontal resultant. That is, the longer the horizontal resultant, the more the A-P dimension must be increased. The position of the base of support, however, is always at right angles to the horizontal resultant.
The horizontal resultant is the net effect of the direction of the forces required to restore normal position and equilibrium to the C-1 subluxation complex. The length of the resultant varies with the magnitude of the height (vertical) and rotation (horizontal) vectors which are computed from the x-ray films. The longer the horizontal resultant, the more conversion of the adjuster’s body to a vertical plane is required to accommodate to the subluxation’s larger misalignment factors; thus the A-P distance of the base must be increased. The width of the base is established by the distance between the adjuster’s acetabular cavities. In all subluxations, however, the base of support is positioned one inch from the distal end of the horizontal resultant and one inch beyond it. This is the reference point and is called the settleback point (see Fig. 3).
The location of the center of gravity of the body shifts when the body parts move.14 When performing the potential phases of the C-1 adjustment, the adjuster moves about several joint axes of motion which vary, of course, in different phases. To control his center of gravity, the adjuster must know and be aware of each joint center of motion and the degree of movement permitted in each act.
For example, in the first or approach phase the adjuster’s mind must be concentrated on his acetabulum on the side of the leg which he places forward in establishing the A-P distance of the base of support. He must move solely from that joint, not permitting his lumbosacral joint to become involved in the act. In the second, or settleback phase, the adjuster’s concentration must be on his acetabula as the centers of motion about which he moves his body backward as if down an inclined plane. In the turn-in phase, the adjuster turns his episternal notch over the contact point from the ankle joint centers of motion, using the rotatores of his legs to turn the body. In the conversion phase which brings the adjuster’s episternal notch back to the settleback point on the horizontal resultant, the center of motion takes place about an external reference point -the contact point- with which the adjuster’s episternal notch is aligned. Each of these movements shifts the adjuster’s center of gravity, and if any act is not performed from the correct joint center of motion and to the correct degree, the adjustic action lines or parallel forces will not be coplanar with the reduction pathway.
As the adjuster settles back at right angles to the horizontal resultant, his center of gravity tends to move toward the back of his base of support. Therefore, he loses stability; his weight is too far back on his heels. The remedy is to increase the A-P distance of the base of support by advancing the forward foot still more. This action brings the adjuster’s center of gravity forward, restoring stability.
The remedy is effective if the base of support is correctly situated in relation to the horizontal resultant. Sometimes the base of support is established too far forward toward the horizontal resultant. More frequently, however, it is too far back from the horizontal resultant. In either case, the adjuster must start over, and reestablish his base. With some experience the procedure becomes automatic.
A guide to correctly establishing a base of support is to align it with the horizontal resultant. The adjuster notes where the horizontal resultant would pass, if extended, and places his forward foot in a position where the extended portion of the horizontal resultant would pass through the arch of his forward foot (see Fig. 3).
A problem often encountered by adjusters in the settleback phase is that of assumed inflexibility of back musculature. In settling back they reach a point where they can no longer continue the action. If they will consciously relax the back and pelvic musculature and permit the pelvis to turn still more vertically, they will considerably increase their settleback action. It is not the muscular inflexibility that creates the problem, but the failure of the pelvic girdle to assume a more vertical plane.
Conversion or angulation of the adjuster’s body to a more vertical plane is an essential element in aligning the parallel forces with the reduction pathway. Conversion of the pelvic and shoulder levers takes place in the second, or settleback phase, and is caused by advancing the leg to conform to the A-P dimension of the base of support. Greater conversion occurs in the sixth or conversion phase. The procedure for executing the conversion phase is for the adjuster, immediately following roll-in and contact, to visualize a line from his shoulder on the side of his contact hand to the opposite hip. Along this imaginary line, the adjuster settles his body backward, allowing his shoulder and hip levers to turn to a more vertical plane as he does so.
The more the adjuster converts his body, the closer his center of gravity will approximate his forward foot. This action may be likened to tipping any elongated object; the line of gravity of the object always falls to the side of the base of support to which the object is tipped.

Figure 4a: Location of adjuster’s center of gravity in Phases 1, 2, and in the final phase.
The adjuster starts to control his center of gravity in the first or approach phase, keeping it close to the distal side of his base or near his forwardly placed foot (Fig. 4a). As he settles back he maintains this relationship of gravity, or weight, to the base of support. In turning his body to bring his episternal notch over the contact point, the adjuster’s center of gravity will shift to the proximal side of the base (Fig. 4b). As he executes the conversion or sixth phase, the adjuster’s center of gravity will return to the distal side of the base. The greater the angulation or conversion of the adjuster’s pelvic and shoulder levers, the faster will the center of gravity return to its original position.
Failure to properly angulate or convert the adjuster’s body planes will increase laterality of C-1 in cases requiring a high or vertical vector. The spinous process of C-2 may rotate farther to the side of laterality, and subjacent vertebrae become more greatly misaligned. Cases necessitating a long rotation vector may result in still longer rotations.
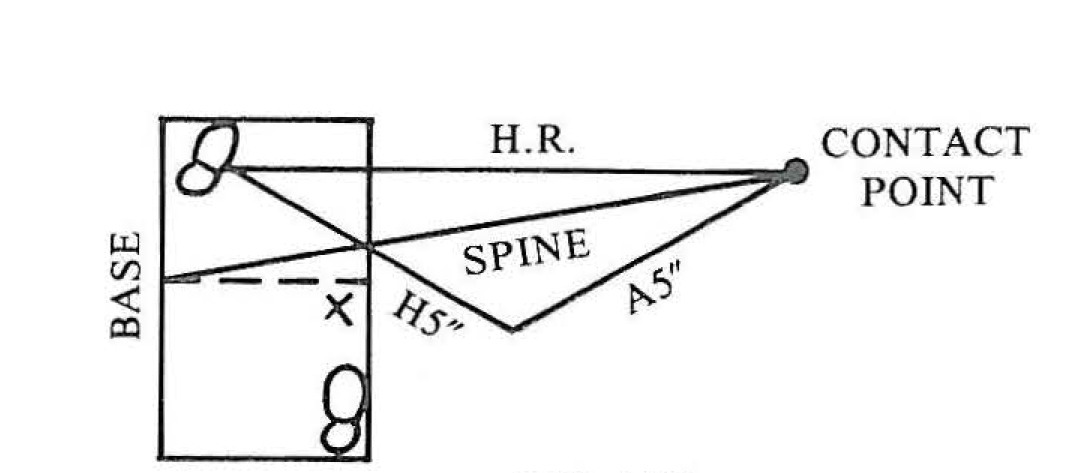
Figure 4b: Location of adjuster’s center of gravity in Phase 3 (turn-in phase) after turning spinal lever over contact point.
Instability from any cause produces curvilinear motion. Parallel forces exist when the action lines of the adjustment parallel each other in time and in distance. Subluxation-reduction takes place only when the action lines from the adjuster’s episternal notch and pelvic center of gravity align exactly with the reduction pathway. When this alignment is accomplished, the adjustic motor skill has been efficiently performed and maximal reduction of the subluxation’s misalignment factors easily obtained.
FOLLOW-THROUGH
Follow-through in the adjustic motor skill is a continuation of the momentum generated by the triceps as they overcome the inertia of the adjuster’s body. The activation of the adjuster’s pectoral girdle transfers momentum to the adjuster’s body, and a “pull” into the adjustment along the reduction pathway is experienced. This pull may be likened to the suction one feels when standing too close to a speeding train. The pull is not a body-drop which is initiated from the lumbo-sacral joint and which would introduce curvilinear motion, destroying the alignment of the parallel forces to the reduction pathway. Follow-through is a drawing of the adjuster’s spinal lever into the adjustment in which the adjuster’s episternal notch and pelvic center of gravity, the sources of his parallel forces, move the same distance along the reduction pathway at the same time.
An adjustment involves movement at many body joints. Several anatomic levers, therefore, contribute to the production of adjustic force. The principle of the continuity of motion states that when a sequence of movements is employed in any motor skill, there should be no pause between them.15 That is to say, a fluid or uninterrupted motion should take place if efficiency is to be obtained, because a break in the continuity of motion reduces the force and momentum generated by the action of the levers.
A violation of the principle of the continuity of motion occurs when an adjuster’s triceps do not contract equally. One muscle, usually the one on the side of the contact hand, contracts slower than the one on the side of the roll-in hand. The force and momentum of the pectoral girdle is reduced because the total motion is interrupted. This error will be reflected in the post x-rays by a loss of equal reduction in the subluxation’s misalignment factors. That is, laterality and rotation will not reduce equally.
An effective completion of the adjustic action requires follow-through. If the adjuster prevents his spinal lever from continuing the action initiated by his triceps brachii contraction, effectiveness is decreased because the effect of the adjustic motion is shortened.
Follow-through also provides time (for the adjuster) to perceive feedback information.16
FEEDBACK
Feedback, or kinesthesis (kinesthesia), according to Dorland’s Medical Dictionary (1965), is the sense by which muscular motion, weight, position, etc. are perceived. To the adjuster, kinesthesis is his ability to perceive, or be aware of through his senses, his muscle and joint movements, the relative alignment of his body parts in space, and the distribution of his body weight. When the adjuster has “learned” to visualize the relative positions of his shoulder and pelvic levers in a given subluxation, and to perceive his parallel forces in relation to the reduction pathway, he will have automatically resolved most of his problems.
To master feedback requires concentration. To utilize it effectively the adjuster should make it a habit to practice with a subluxation listing. Different listings should be used. Following this procedure, the adjuster will eventually be able to “see” the position of his spinal, shoulder, and pelvic levers and to judge the accuracy of his parallel forces. The coordinator rubber top, as it moves, will tell him if the direction of his parallel forces aligns with the reduction pathway of the listing he is addressing. Feedback from the coordinator top will also tell him as it moves if he is expressing curvilinear motion. If the adjuster finds that he is expressing curvilinear motion, his base of support is probably not aligned to the horizontal resultant at the settleback point, or he is not converting his body planes correctly, or is not locking his pelvis on the side of the forward leg. Another error that can cause the curvilinear problem is an incorrect relationship between the adjuster’s center of gravity and base of support.
The manner in which the coordinator top depresses provides reliable feedback. Too frequently the rubber top moves straight downward. When this occurs it is obvious that the adjuster’s parallel forces are not aligned to the reduction pathway, probably because of too little conversion of the adjuster’s body planes. This error is corrected by increasing the A-P dimension of the base of support, by locking the hip on the side of the forward leg, or by correcting any unequal contraction of the triceps brachii. These errors can also cause the rubber top to move toward the adjuster.
If these errors occur in practice, they can also take place when adjusting a patient’s subluxation, increasing the subluxation’s misalignment factors and traumatizing the patient.
Feedback permits the adjuster to analyze his performance, and to make corrections where necessary. It is through his receptors that the adjuster receives input concerning his performance of the motor skill, and it provides the means whereby he improves his art.
CONCLUSIONS
This paper discusses the C-1 adjustment as a motor skill, subject in its performance to the relevant kinesiological principles and concepts that govern a motor skill. This paper suggests how upper cervical adjusters might improve their level of performance through a more complete understanding and proper application of these principles. The need to treat the C-1 subluxation as separate from those subluxations of subjacent vertebrae because of biomechanical and kinesiological reasons is also indicated. Perhaps not stressed enough is the potential danger to the patient who receives upper cervical manipulative systems that violate the proposed mechanical laws discussed in this article.
The neurological and biomechanical rationale of the C-1 subluxation is mentioned, and the need for every chiropractor (and other health practitioners) to precisely and accurately restore the misalignments of the C-1 subluxation complex to normal. Every patient with a distorted pelvis and unbalanced spine possesses a C-1 subluxation, and the correction of these structures cannot be accomplished until the C-1 subluxation is normalized.
The concept of adjustic force and its control discussed in this article differs greatly from adjustic force concepts now taught and practiced in the colleges. Other concepts, i.e., motion, reflexes, base of support, center of gravity, parallel forces, follow-through, and feedback are sufficiently discussed to help the practitioner become a more efficient adjuster.
While this paper does not include a full mechanical analysis, it is hoped this discussion will arouse some interest in proper adjusting. The value of the essential nature of chiropractic the subluxation and its correction (adjustment) – depends upon a continuing study of the adjustic motor skill, and the development of improved methods of adjusting. Such a study and analysis, aside from improving the performance of the adjuster, more highly motivates him. It also provides added protection to the patient.
REFERENCES:
1. White, A. A. & Panjabi, M. M., Clinical Biomechanics of the Spine, J. B. Lippincott Co., Philadelphia, 1978.
2. Steindler, A., Kinesiology of the Human Body, 5th Edition, Charles C. Thomas. Springfield, 1977. P. 145.
3. White, A. A. & Panjabi, M. M., Clinical Biomechanics of the Spine, J. B. Lippincott Co., Philadelphia , 1978.
4. Seemann, D. C., C-1 Subluxations, Short Leg and Pelvic Distortions, Upper Cervical Monograph, Volume 2, Number 5, November, 1978.
5. Gowitzke, B. A. & Milner, M., Understanding the Scientific Basis of Human Motion, 2nd Edition, Williams & Wilkins Co., Baltimore, 1980. P. 317.
6. Rasch, P. J. & Burke, R. K., Kinesiology and Applied Anatomy, 5th Edition, Lea & Febiger, Philadelphia, 1974. P. 136.
7. Anderson, T. McClurg, Human Kinetics and Analyzing Body Movements, William Heinemann Medical Books Ltd., London, 1951. Pp. 94-98.
8. Groves, R. & Camaione, D. N., Concepts in Kinesiology, W. B. Saunders Co., Philadelphia, 1975, p. 35.
9. Ibid., p. 53.
10. Ibid., p. 135.
11. lbid., p. 71.
12. lbid., p. 183.
13. lbid., p. 259.
14. Ibid., p. 161.
15. Ibid., p. 209.
16. lbid., p. 257.